Gastrointestinal Diseases
The gastrointestinal tract consists of the esophagus, stomach, small intestine, and large intestine, and is a vital organ system responsible for digestion, absorption, and excretion. Among these, tumor lesions that occur in the gastrointestinal tract often lack subjective symptoms in the early stages, and delays in detection can greatly affect prognosis, so accurate diagnosis and appropriate therapeutic intervention are extremely important.
The Department of Gastrointestinal Cancer offers multidisciplinary treatment based on the latest evidence for malignant tumors of the digestive tract including esophageal cancer, gastric cancer, and colorectal cancer, as well as precancerous lesions and benign tumors such as adenoma and submucosal tumor, by performing precise diagnosis mainly through endoscopy, and by collaborating with related departments and local medical institutions for treatment from endoscopic therapy to pharmacological therapy. We provide multidisciplinary treatment based on the latest evidence in collaboration with related departments and local medical institutions. Especially in endoscopic diagnosis and treatment, we emphasize qualitative diagnosis and depth assessment of lesions, aiming at minimally invasive and highly curative treatment. In addition to organic diseases, we also provide appropriate evaluation for functional gastrointestinal disorders such as functional dyspepsia and irritable bowel syndrome, including exclusion of organic diseases, and treatment with consideration of symptoms and life background.
For early-stage esophageal cancer, we actively perform minimally invasive treatment using endoscopic submucosal dissection (ESD). For advanced cancer, we collaborate with the Department of Surgery and the Department of Radiology to select a treatment method that best suits the patient's condition, such as chemoradiation therapy combining anticancer drugs and radiation therapy.
We strive for accurate diagnosis and early detection of lesions by utilizing image-enhanced endoscopy (IEE), magnification, and ultrasound endoscopy. For treatment, in addition to minimally invasive treatment by ESD, treatment for unresectable or recurrent gastric cancer is selected based on gene-related tests (biomarker tests) and drug therapy using chemotherapy, molecular targeted drugs, and immune checkpoint inhibitors.
For small adenomas, we actively perform submersion endoscopic mucosal resection (UEMR). ESD is also performed for suspicious or large lesions, and joint duodenal-laparoscopic endoscopic colectomy (D-LECS) is performed with the Department of Surgery for high-risk cases.
We perform many endoscopic resections (EMR/ESD) for colorectal polyps and early-stage colorectal cancer. For advanced cancer, treatment is selected based on gene-related tests, and chemotherapy using molecular targeted drugs and immune checkpoint inhibitors is performed.
For rare tumors such as small intestine cancer, GIST (gastrointestinal stromal tumor), and NET (neuroendocrine tumor), we use ultrasound endoscopy, capsule endoscopy, double-balloon small bowel endoscopy, and other testing equipment to diagnose and provide specialized treatment. For neuroendocrine tumors, peptide receptor radionuclide therapy (PRRT) is performed in collaboration with the Isotope Therapy Center.
We also provide detailed pathological evaluation and meticulous treatment for diseases such as functional dyspepsia (FD) and irritable bowel syndrome (IBS), in which no organic abnormality is found but painful symptoms accompany the disease.
We actively perform minimally invasive treatment, mainly endoscopic submucosal dissection (ESD), for early-stage gastrointestinal cancers of the esophagus, stomach, duodenum, and large intestine. Prior to treatment, we use the latest generation endoscopic models and high-performance light sources for precise observation, and evaluate the qualitative and depth diagnosis of lesions with high precision using magnification, image-enhanced endoscopy, and ultrasound endoscopy. We then discuss the treatment plan for each patient according to his or her individual condition in full consultation with multiple disciplines, including surgery.
ESD is a difficult procedure that requires advanced techniques and extensive experience, while enabling accurate pathological diagnosis and achieving both radical cure and organ preservation by resecting the lesion en bloc. We perform ESD on all gastrointestinal organs except the pharynx, including the esophagus, stomach, duodenum, and large intestine, and actively perform endoscopic treatment for cases that are generally considered difficult, such as giant lesions, highly fibrotic lesions, recurrent lesions after treatment, and supradiverticular lesions. We also perform ESD under general anesthesia in the operating room for patients at risk of airway stricture, lesions in the cervical esophagus, and duodenal cancer. We are constantly striving to improve safety and outcomes through our abundant case experience, established techniques, and perioperative management.
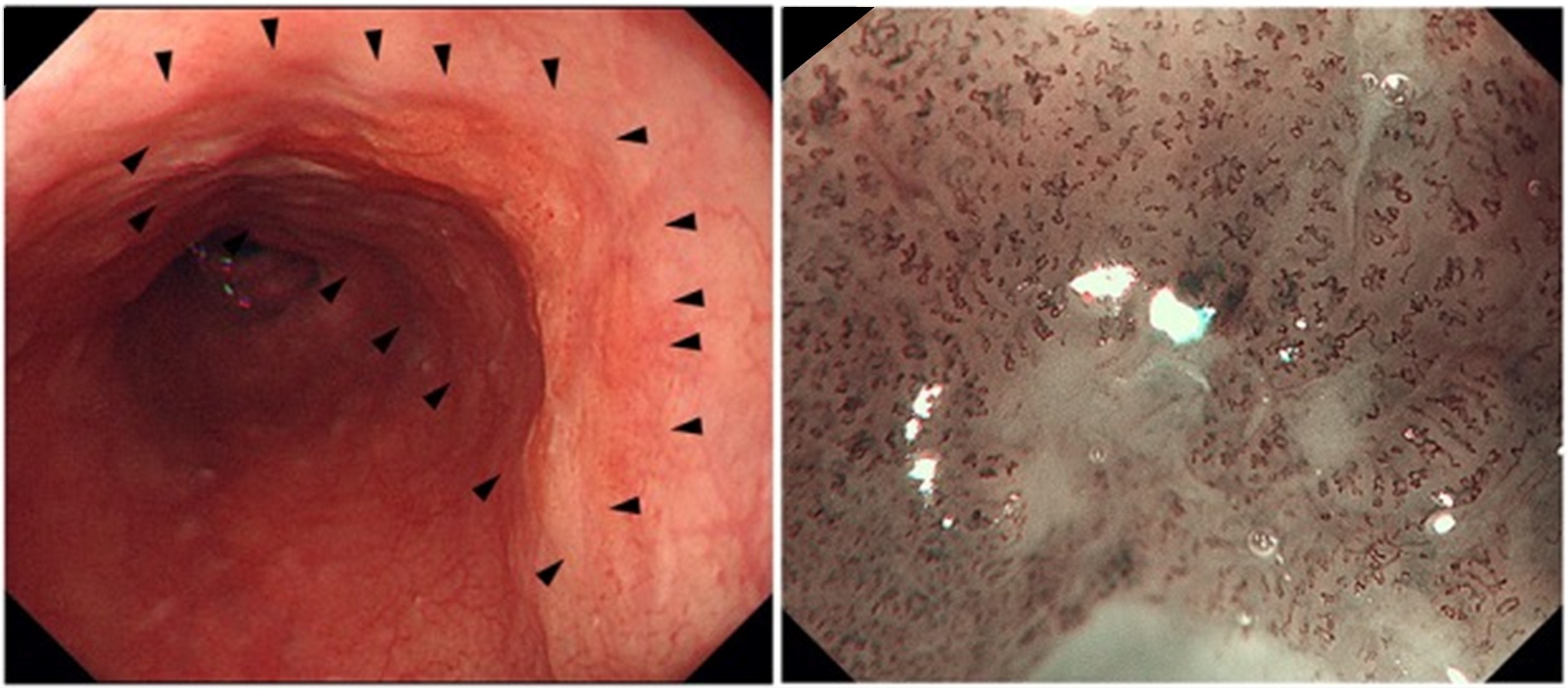 Figure 1: Diagnosis of esophageal cancer depth using magnifying endoscope
Figure 1: Diagnosis of esophageal cancer depth using magnifying endoscope
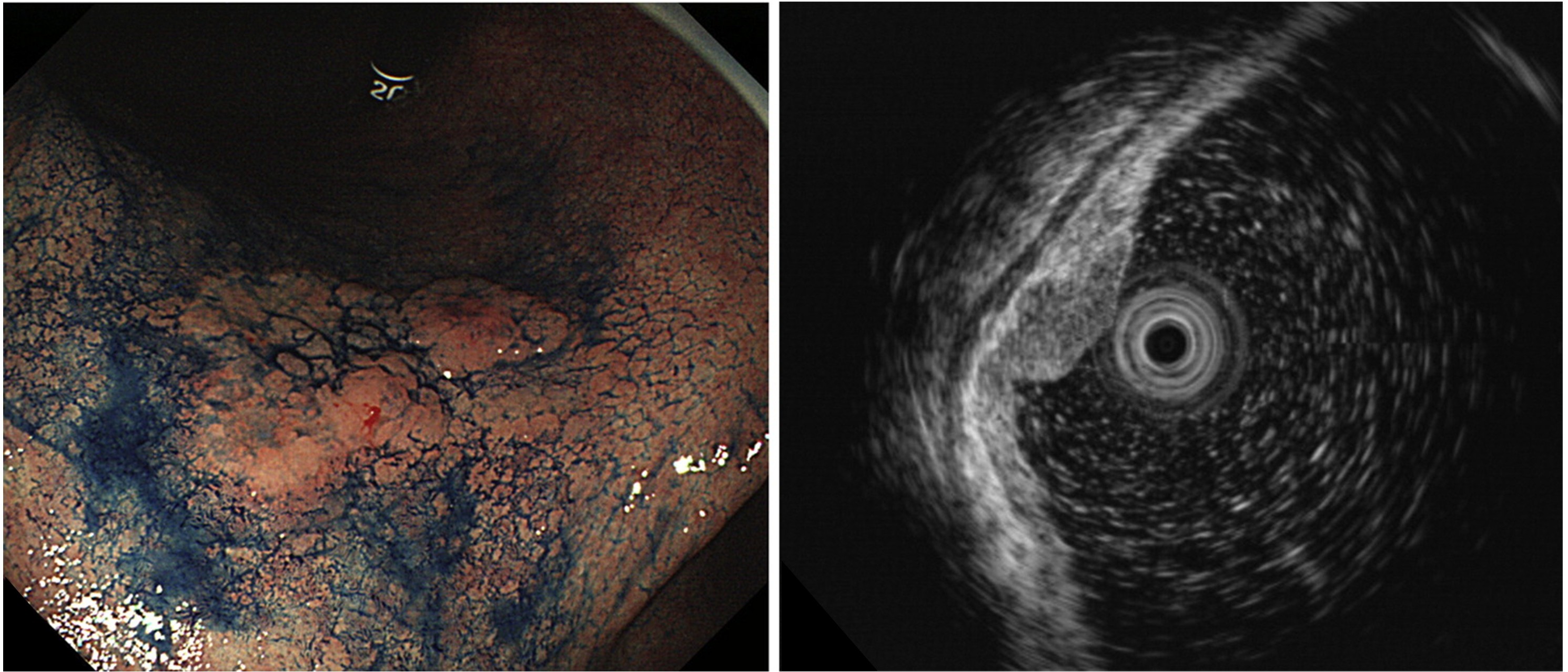 Figure 2: Diagnosis of gastric cancer depth using ultrasound endoscopy
Figure 2: Diagnosis of gastric cancer depth using ultrasound endoscopy
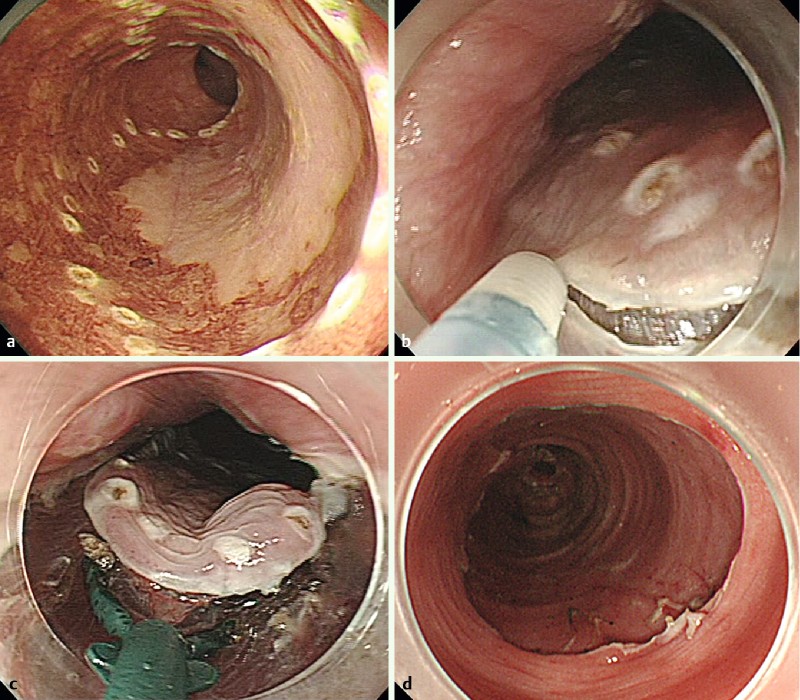 Figure 3: Endoscopic submucosal dissection (ESD) for esophageal cancer
Figure 3: Endoscopic submucosal dissection (ESD) for esophageal cancer
We practice chemotherapy for unresectable gastrointestinal cancers based on the latest domestic and international evidence. For esophageal, gastric, colorectal, and other cancers, we provide standard treatments including molecular-targeted agents and immune checkpoint inhibitors, and develop treatment strategies according to the patient's general condition and tumor characteristics. We also provide treatment for high-risk patients with special underlying diseases such as collagen disease, post-transplantation, heart failure, liver cirrhosis, severely impaired renal function, and dialysis, in collaboration with specialized departments.
As one of the 13 "Core Base Hospitals for Cancer Genome Medicine" designated nationwide, we actively incorporate gene panel testing into our routine medical care. This enables us to participate in clinical trials and trials based on genetic abnormalities in addition to standard treatments, providing new treatment options for patients. Genomic information is carefully reviewed by a team of experts, and treatment proposals are based on scientific evidence.
In addition, we hold regular weekly conferences with the Department of Gastroenterological Surgery to discuss the possibility of conversion surgery for advanced cancer with distant metastasis or unresectable locally advanced cancer after tumor reduction by chemotherapy. Through close collaboration between internal medicine and surgery, we pursue multidisciplinary treatment aiming for cure as much as possible, even in cases judged to be "unresectable.
For patients with gastrointestinal transit disturbance, we also focus on supportive care with an emphasis on maintaining quality of life. Endoscopic stenting, endoscopic gastrostomy (PEG), and endoscopic balloon dilation for gastrointestinal stenosis due to postoperative scarring are actively performed. Percutaneous transesophageal gastroesophageal tube insertion (PTEG) is also performed in collaboration with the Department of Radiology and IVR for patients who have difficulty in PEG creation after abdominal surgery. For patients who have difficulty with the endoscopic approach, CT-guided gastrostomy is also available, and we provide a flexible approach according to the patient's condition.
We provide specialized care not only for organic diseases, but also for functional gastrointestinal diseases, which are mainly abnormalities in the motility and function of the gastrointestinal tract. In cases where severe reflux esophagitis, achalasia, or esophageal motility disorder is suspected, 24-hour pH monitoring and high-resolution intraesophageal pressure testing are performed in collaboration with the Department of Surgery. After objectively evaluating the cause of symptoms with these tests, we consider a treatment plan that includes drug therapy, endoscopic therapy, and surgical treatment. For patients with severe reflux esophagitis, we offer endoscopic anti-reflux mucosal surgery (ARMS) and surgical anti-reflux surgery using the Nissen method.
For achalasia, the department does not perform oral endoscopic myotomy (POEM), but does perform balloon dilation of achalasia for those cases in which it is necessary. In collaboration with the Department of Surgery, surgical treatment using the Heller-Dor procedure is also available. Furthermore, for those cases in which POEM is deemed optimal, we ensure the best treatment opportunity for the patient by appropriately referring the patient to a facility that specializes in POEM.
On the other hand, for cases of intestinal dysfunction such as chronic pseudo intestinal obstruction (CIPO), we provide treatment under multidisciplinary cooperation centering on the Intestinal Insufficiency Center. While symptomatic treatment is the basis of treatment, surgery is considered depending on the condition, and nutritional therapy including home central venous nutrition (TPN) is combined to provide comprehensive medical care with an emphasis on long-term quality of life.