Gastrointestinal Cancer and Endoscopy Group
Group Leader: Yoshiki Tsujii
Concept: Integrating endoscopy and science to create the future of gastrointestinal cancer treatment
Combining advanced clinical skills and scientific thinking based on endoscopic care, we strive to generate evidence directly related to clinical practice in order to contribute to the advancement of diagnosis and treatment of gastrointestinal cancers. We conduct a wide range of research, from basic to clinical, to elucidate the mechanisms of development and progression of gastrointestinal cancers, search for new therapeutic targets and useful biomarkers, and develop highly accurate diagnostic techniques and minimally invasive therapies. Furthermore, based on research organizations such as OGF (Osaka Gut Forum), we are actively promoting multicenter collaborative research and returning the results to clinical practice in order to realize higher quality medical care.
Pursuit of qualitative improvement in the treatment of gastrointestinal cancers centered on endoscopy
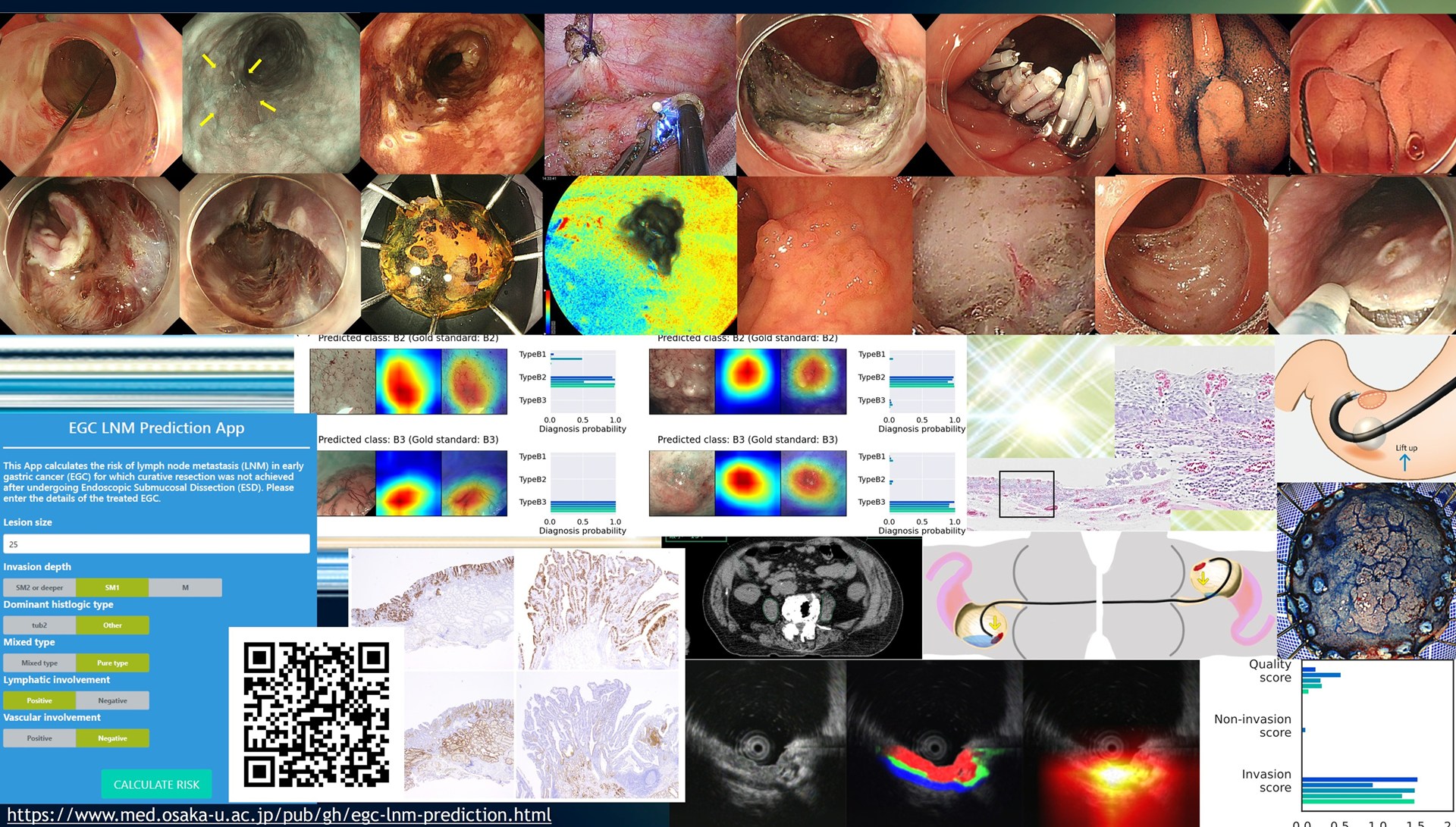
Accurate diagnosis and selection of appropriate therapeutic measures are essential to improve the outcome of endoscopic treatment for early-stage gastrointestinal cancers, especially ESD. Therefore, we aim to develop high-precision diagnostic techniques and establish optimal treatment strategies based on high-precision diagnosis. Furthermore, in order to achieve safe and reliable radical cure, we are striving to refine our techniques and develop new, less invasive endoscopic therapies. In addition to endoscopic treatment, we are pursuing qualitative improvement of cancer treatment by maximizing the use of clinical specimens and data obtained in the process of multidisciplinary treatment using various drug therapies and radiotherapy based on biomarker measurement and gene panel testing, and also by utilizing AI. We have reported on studies on diagnosis of gastrointestinal cancers1-3), evaluation of minimally invasive treatment methods for gastrointestinal cancers4-5) and development of new treatments6-7), and studies on multidisciplinary treatment8-9).
Generating real-world evidence through multicenter collaborative research
Taking clinical questions generated from clinical practice as our starting point, we actively promote multicenter collaborative research to solve current clinical problems. Our group has established a strong network with Osaka University-affiliated facilities and is leading multifaceted research using the OGF (Osaka Gut Forum) as a research platform to generate and disseminate evidence. So far, we have reported the construction of an AI-based EUS depth diagnostic model10) and a lymph node metastasis prediction model11) , advocated measures to prevent bleeding after ESD12) , verified long-term results after ESD13-14) , and examined the developmental progression of duodenal adenomas15).
Deepening basic and bridging research rooted in endoscopic practice
We are conducting basic and bridging research to elucidate the mechanisms of development and progression of gastrointestinal cancers and to search for novel therapeutic targets and useful biomarkers through clinicopathological and molecular biological analyses. We have previously reported the identification of factors that make the diagnosis of gastric cancer difficult16) and the mechanisms of cancer cell-stromal interactions that promote the progression of colorectal cancer17-20).
Future Prospects: Toward the Era of Controlling Gastrointestinal Cancers - Integrated Evolution of Diagnosis, Treatment, and Prediction
We aim to improve and optimize the quality of gastrointestinal cancer care through further scientific development of diagnosis and treatment centered on endoscopy, establishment of a multilayered diagnostic system integrating AI diagnosis and biomarkers, and development of new therapeutic targets and biomarkers. By further strengthening our multicenter collaborative research network and developing findings from observational studies into prospective intervention studies, we will generate evidence to change medical practice and transform gastrointestinal cancer into a "controllable disease.
Major Papers
- Tsujii Y, Hayashi Y, Ishihara R, Yamaguchi S, Yamamoto M, Inoue T, Nagai K, Ogiyama H, Yamada T, Nakahara M, Kizu T, Kanesaka T, Matsuura N, Ohta T, Nakamatsu D, Yoshii S, Shinzaki S, Nishida T, Iijima H, Takehara T. Diagnostic value of endoscopic ultrasonography for the depth of gastric cancer suspected of Surg Endosc. 2023 Apr;37(4):3018-3028.
- Uema R, Hayashi Y, Tashiro T, Saiki H, Kato M, Amano T, Tani M, Yoshihara T, Inoue T, Kimura K, Iwatani S, Sakatani A, Yoshii S, Tsujii Y, Shinzaki S, Iijima H, Takehara T. Use of convolutional neural networks for classifying microvessels of superficial esophageal squamous cell carcinomas. Takehara T. Use of a convolutional neural network for classifying microvessels of superficial esophageal squamous cell carcinomas. Hepatol. 2021 Aug;36(8):2239-2246.
- Tsujii Y, Kato M, Inoue T, Yoshii S, Nagai K, Fujinaga T, Maekawa A, Hayashi Y, Akasaka T, Shinzaki S, Watabe K, Nishida T, Iijima H, Tsujii M, Takehara T. Integrated diagnostic strategy for the invasion depth of early gastric cancer by conventional endoscopy and EUS. Gastrointest Endosc. 2015 Sep;82(3): 452-9. 452-9.
- Adachi Y, Hayashi Y, Yoneda S, Tajiri A, Fukuda H, Kimura E, Nakagawa K, Saiki H, Uema R, Yoshihara T, Tsujii Y, Takehara T. Outcomes of additional Outcomes of additional chemotherapy for esophageal squamous cell carcinoma following non-curative endoscopic submucosal dissection. Int J Clin Oncol. 2025 Dec;30(12): 2567-2575. 2567-2575.
- Tsujii Y, Hayashi Y, Uema R, Saiki H, Kimura E, Nakagawa K, Fukuda H, Tajiri A, Adachi Y, Yoshihara T, Inoue T, Kato M, Yoshii S, Suzuki M, Makino T, Takehara T. Feasibility and safety of endoscopic submucosal dissection for superficial cancer of the remnant esophagus after esophagectomy. Esophagus. 2025 Apr; 22(2):148-156.
- Tsujii Y, Yamasaki M, Hayashi Y, Tanaka K, Makino T, Doki Y, Takehara T. Thoracoscopic and endoscopic cooperative surgery (TECS): a novel less invasive technique for resection of gastric tube cancer after esophagectomy. endoscopy. 2019 Jan;51(1):E5-E6.
- Yoshii S, Akasaka T, Hayashi Y, Tsujii Y, Nagai K, Higashino K, Ishihara R, Iijima H, Takehara T. “Underwater” endoscopic submucosal dissection: a novel method for resection in saline with a bipolar needle knife for colorectal epithelial neoplasia. Surg Endosc. 2018 Dec;32 (12):5031-5036.
- Nakagawa K, Hayashi Y, Adachi Y, Tajiri A, Fukuda H, Kimura E, Uema R, Saiki H, Kato M, Inoue T, Yoshihara T, Yoshii S, Tsujii Y, Takehara T. Low skeletal Esophagus. 2025 Apr;22(2):19:19-25 Apr;22(2):198-206.
- Hayashi Y, Iijima H, Isohashi F, Tsujii Y, Fujinaga T, Nagai K, Yoshii S, Sakatani A, Hiyama S, Shinzaki S, Makino T, Yamasaki M, Ogawa K, Doki Y, Takehara T. The heart's exposure to radiation increases the risk of cardiac toxicity after chemoradiotherapy for superficial esophageal cancer: a retrospective cohort study. retrospective cohort study. BMC Cancer. 2019 Mar 4;19(1):195.
- Uema R, Hayashi Y, Kizu T, Igura T, Ogiyama H, Yamada T, Takeda R, Nagai K, Inoue T, Yamamoto M, Yamaguchi S, Kanesaka T, Yoshihara T, Kato M, Yoshii S, Tsujii Y Shinzaki S, Takehara T. A novel artificial intelligence-based endoscopic ultrasonography diagnostic system for diagnosing the invasion depth of J Gastroenterol. 2024 Jul;59(7):543-555.
- Kato M, Hayashi Y, Uema R, Kanesaka T, Yamaguchi S, Maekawa A, Yamada T, Yamamoto M, Kitamura S, Inoue T, Yamamoto S, Kizu T, Takeda R, Ogiyama H, Yamamoto K, Aoi K, Nagaike K, Sasai Y, Egawa S, Akamatsu H, Ogawa H, Komori M, Akihiro N, Yoshihara T, Tsujii Y, Takehara T Aoi K, Nagaike K, Sasai Y, Egawa S, Akamatsu H, Ogawa H, Komori M, Akihiro N, Yoshihara T, Tsujii Y, Takehara T. A machine learning model for predicting the Gastric Cancer. 2024 Sep;27(5):1069-1077.
- Ogiyama H, Kato M, Yamaguchi S, Kanesaka T, Yamada T, Yamamoto M, Komori M, Nagaike K, Nakahara M, Tsutsui S, Tsujii Y, Saita R, Iijima H, Hayashi Y, Takehara T. Efficacy of prophylactic clip closure in reducing the risk of delayed bleeding after colorectal endoscopic submucosal dissection in patients on Dig Endosc. 2024 Sep;36(9):1021-1029.
- Tajiri A, Tsujii Y, Nishida T, Inoue T, Maekawa A, Kitamura S, Yamaguchi S, Nishihara A, Yamada T, Ogiyama H, Murayama Y, Yamamoto S, Egawa S, Uema R, Yoshihara T, Hayashi Y, Takehara T. Yoshihara T, Hayashi Y, Takehara T. High incidence of lung cancer death after curative endoscopic submucosal dissection for superficial esophageal Cancer Med. 2024 May;13(9):e7242.
- Kato M, Hayashi Y, Fukuda H, Yamaguchi S, Inoue T, Ogiyama H, Kitamura S, Komori M, Yamamoto K, Yamamoto M, Nagai K, Nakahara M, Egawa S, Yamada T, Sasakawa A, Kizu T, Nishiyama O, Shichijo S, Yoshii S, Tsujii Y, Shinzaki S, Iijima H, Takehara T. Geriatric nutritional risk index as a prognostic indicator Kizu T, Nishiyama O, Shichijo S, Yoshii S, Tsujii Y, Shinzaki S, Iijima H, Takehara T. Geriatric nutritional risk index as a prognostic indicator in Geriatric nutritional risk index as a prognostic indicator in elderly patients with early colorectal cancer undergoing endoscopic submucosal dissection. Dig Endosc. 2022 Mar;34(3):569-578.
- Uema R, Hayashi Y, Komori M, Shibukawa N, Hayashi N, Horimoto M, Yamada T, Yamamoto M, Hiyama S, Kinoshita K, Ogiyama H, Yamaguchi S, Egawa S, Kanesaka T, Kato M, Yoshii S, Tsujii Y, Keiichiro H, Shinzaki S, Iijima H, Morii E, Takehara T. Kato M, Yoshii S, Tsujii Y, Keiichiro H, Shinzaki S, Iijima H, Morii E, Takehara T. Non-Pure Intestinal Phenotype as an Indicator of Progression in Sporadic Nonampullary Duodenal Adenomas: A Multicenter Retrospective Cohort Study. Clin Transl Gastroenterol. 2024 Jan 1;15(1):e00649.
- Nagai K, Hayashi Y, Uema R, Inoue T, Kimura K, Sakatani A, Yoshii S, Tsujii Y, Shinzaki S, Iijima H, Takehara T. Clinical and Histopathological Features of the Differentiated Type of Early Gastric Cancer with an Unclear Lateral Demarcation. Clinical and Histopathological Features of the Differentiated Type of Early Gastric Cancer with an Unclear Lateral Demarcation. Digestion. 2022;103(5):347-356.
- Kimura E, Hayashi Y, Nakagawa K, Saiki H, Kato M, Uema R, Inoue T, Yoshihara T, Sakatani A, Fukuda H, Tajiri A, Adachi Y, Murai K, Yoshii S, Tsujii Y, Shinzaki S Iijima H, Takehara T. p53 Deficiency in Colon Cancer Cells Promotes Tumor Progression Through the Modulation of Meflin in Fibroblasts. Jul;116(7):1871-1882.
- Saiki H, Hayashi Y, Yoshii S, Kimura E, Nakagawa K, Kato M, Uema R, Inoue T, Sakatani A, Yoshihara T, Tsujii Y, Shinzaki S, Iijima H, Takehara T. The apelin The apelin receptor signaling pathway in fibroblasts is involved in tumor growth via p53 expression of cancer cells. Int J Oncol. 2023 Dec;63(6):139.
- Inoue T, Hayashi Y, Tsujii Y, Yoshii S, Sakatani A, Kimura K, Uema R, Kato M, Saiki H, Shinzaki S, Iijima H, Takehara T. Suppression of autophagy promotes fibroblast activation in p53-deficient colorectal cancer cells. Sci Rep. 2021 Sep 30;11(1):19524.
- Yoshii S, Hayashi Y, Iijima H, Inoue T, Kimura K, Sakatani A, Nagai K, Fujinaga T, Hiyama S, Kodama T, Shinzaki S, Tsujii Y, Watabe K, Takehara T. Exosomal microRNAs derived from colon cancer cells promote tumor progression by suppressing fibroblast TP53 expression. Cancer Sci. 2019 Aug;110(8):2396- 2407.